
LUIS E. ZEA-SALAZAR
Department of Pediatric Surgery, Hospital del Niño
"Francisco de Ycaza Bustamante," Guayaquil, Ecuador.
Abstract. A modification to the Posterior sagittal anorectoplasty technique, developed by A. Peña is described. A down based rectal flap makes it easier to reach the new anus, without dissecting the ventral side of the rectal pouch, and uses the tissue otherwise thrown away in the necessary tapering.
Key words: Anorectal anomalies;
Posterior sagittal anorectoplasty; Rectal flap.
Introduction
The posterior sagittal approach developed by A. Peña for the treatment of anorectal anomalies has proved to be the best way of exposure of the anatomy of the perineal region and has been used worldwide with excellent results [1,2,4,7]. However as all other techniques, it implies some kind of tissue damage in the procedure of dissecting around the rectal pouch, with special concern to the external innervation of bowel and low urinary tract [2,7]. The operation discards a portion of rectal tissue in the necessary tapering of the pouch to make an adequate anal canal, that fits in the sometimes not well developed "muscular complex" [1,2,5].
In our hospital, we have modified Dr. Peña's technique,
utilizing the excess of the pouch's wall in the form of a down
based rectal flap. It allows us to reach the new anus site without
mobilizing the ventral side of the terminal bowel; thus preserving
intact it's innervation and vascularization.
FIGURE 1: Lost tissue in Peña"s technique
FIGURE 2: Gained tissue in author"s technique
Materials and method
From our preliminary theoretical considerations, we decided to use this technique on those patients with a high type of anomaly and without a fistula.
We perform the operation as described by Peña [1,2], but on reaching the terminal bowel pouch, we proceed to liberate only its dorsal wall. Dissection of the dorsal wall is taken as far up as possible and necessary, taking into account the length of intestine needed to reach the new-anus.
Then we proceed to delineate the rectal flap, it's length being the same as the distance from the end of the pouch to the new anus, and it's width no less than one third and no more than one half of the circumference of the terminal intestine.
We start to cut the intestine's wall, with the electrocautery, in the middle of the flap's upper limit and then extend the incision to the sides through the hole thickness of the wall. We proceed on both sides toward the distal end. The lateral incisions are stopped about one centimeter before the end of the pouch.

FIGURE 3: Dorsal wall of rectum exposed and flap delimited.
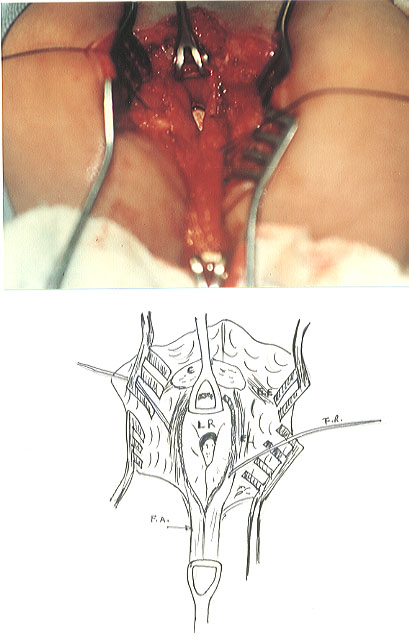
FIGURE 4: Flap swung down.
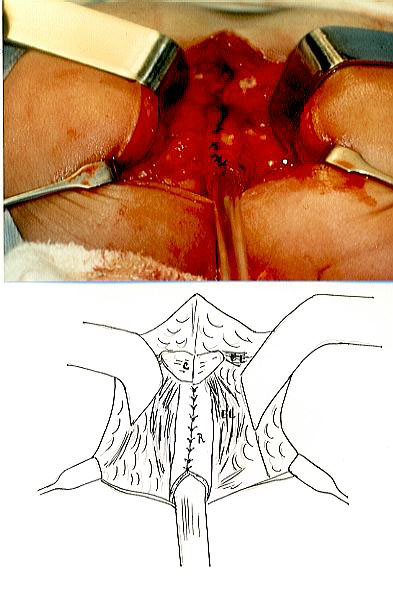
FIGURE 5: Neo rectum formed over a rectal tube.
The flap is swung downwards and the new anus is reached without tension.
We close the intestinal wall over a rectal tube of appropriate
diameter for the age, with two layers of interrupted 4/0 sutures.
The "muscular complex" is re-approximated over the intestinal
tube and the operation completed as described by Peña.
Patients and results
Since 1990 we have used the technique on five patients, two girls and three boys. They all had a high type of anomaly without a fistula. Coincidentally all of them had a Down Syndrome.
|
| ||||
| |||||
|
| ||||
| |||||
|
TABLE 1.- Patients operated with de rectal flap technique.
In all our patients it was easy to reach the new anus site, with an intestinal tube of appropriate caliber. No complication such as isquemia of the flap was present. In case number 2 a high recto-cutaneous fistula developed. It closed spontaneously after two weeks, thanks to the previous diverting colostomy.
The closure of the colostomy was done at least after three months
of rectal dilatation The delay for closing colostomies in Cases
2 and 3 had to do with common problems in our underdeveloped countries,
like malnutrition and insufficient economic resources. All three
patients wich underwent closure of their colostomie acquired early
continence despite their mental handicap proper to their Down
Syndrome. Their mothers related that they usually cried before
stooling and none of them soiled.
TABLE 2.- Rectal Caliber at end of operation and results after
3 to 5 years of follow up. Cases 4 and 5 are not listed because
their colostomy have not been closed yet.
Discussion
The terminal intestine of patients affected with a rectal anomaly is almost always of a great caliber [1,2,5]. Peña and others have stated that it is necessary to taper it [1,2,5] discarding among 30 and 70 percent of the pouch's wall [5]. This tapering is needed to fit the new rectum in the sometimes hipoplasic "muscular complex" [1,2,5].
All the techniques so far developed for the treatment of rectal anomalies have put great concern on preserving the innervation and integrity of other pelvic viscera, specially the genito-urinary tree [2,3,6]. Preservation of the blood supply of the rectal pouch has also been a concern. The extrinsic innervation might be necessary for the maintenance of anal smooth muscle tone[3]. Peña's A.R.P.S.P. lets us view the anatomy of the region and work on it more securely. Although like in any operation: the more we dissect, the more danger there is to damage the innervation and vascularization of the region.
With the rectal flap we describe here, we preserve intact 50% of the extrinsic innervation and vascularization of the rectum and most of all, any damage to de genito-urinary structures bellow is diminish because the ventral wall in not dissected.
References
Article published in Revista de la Federacion de Sociedades de Cirugia Pediatrica del ConoSur, Sept 1994.